Tuesday, November 25, 2008
Tuesday, November 18, 2008
A Case of Obscure Gastrointestinal Bleeding Secondary to a Small Bowel Gastr...
Sent to you by Hemi via Google Reader:
via Medscape Radiology Headlines on 11/18/08
Magnetic resonance enterography may have a role in the evaluation of obscure gastrointestinal bleeding when upper and lower endoscopy is negative and capsule endoscopy is unrevealing. The Medscape Journal of Medicine
Things you can do from here:
- Subscribe to Medscape Radiology Headlines using Google Reader
- Get started using Google Reader to easily keep up with all your favorite sites
Friday, November 14, 2008
Polyp Size and Advanced Histology in Patients Undergoing Colonoscopy
Polyp Size and Advanced Histology in Patients Undergoing Colonoscopy: "In summary, our analysis of asymptomatic patients undergoing colonoscopy screening in diverse clinical settings demonstrates that patients whose largest polyp is 1-5 mm have a very low risk of advanced neoplasia (1.7%), with only rare cases of cancer or high-grade dysplasia. Most of these patients can be safely observed with periodic imaging, assuming that accurate imaging is available. Our study confirms that patients whose largest polyp is ≥10 mm have a high proportion of advanced histology (30.6%). Patients whose largest polyp is 6-9 mm have an intermediate risk of advanced histology (6.6%; range, 4.6%-11.7%) including cancer or high-grade dysplasia in 0.92%. Based on these data, all patients with polyps ≥10 mm, and most patients whose largest polyp is 6-9 mm should receive colonoscopy and polypectomy. This recommendation is now embedded into new colon cancer screening guidelines.[17] Based on our data, 15%-20% of asymptomatic patients would require colonoscopy after imaging studies. These data have important implications for CTC. If large proportions of patients will require colonoscopy after CTC, patients will need to understand the likelihood of requiring colonoscopy and the possible need for 2 bowel preparations. Further study is needed to examine the cost-effectiveness of CTC if 20% of patients will require colonoscopy."
Tuesday, November 11, 2008
Small Colon Polyps: Surgical Removal Is Costly And Unnecessary
Small Colon Polyps: Surgical Removal Is Costly And Unnecessary: "Polypectomy (the surgical removal of polyps by colonoscopy) of small polyps found during CT colonography is costly and unnecessary according to a study performed at the University of Wisconsin School of Medicine and Public Health in Madison, WI.
A decision analysis model was constructed to represent the clinical and economic consequences of performing three year colorectal cancer surveillance, immediate colonoscopy with polypectomy, or neither on patients who have 6-9 mm polyps found on CT colonography (CTC). The analysis model was accompanied by a hypothetical population of 100,000 60-year-old adults with 6- to 9-mm polyps detected at CTC screening. Results showed that, 'by excluding large polyps and masses, CTC screening can place a patient in a very low risk category making colonoscopy for small polyps probably not warranted,' said Perry J. Pickhardt, MD, lead author of the study. 'Approximately 10,000 colonoscopy referrals would be needed for each theoretical cancer death prevented at a cost of nearly $400,000 per life-year gained. We would also expect an additional 10 perforations and probably one death related to these extra colonoscopies. There may be no net gain in terms of lives - just extra costs,' said Dr. Pickhardt.
'The clinical management of small polyps detected at colorectal cancer screening has provoked controversy between radiologists and gastroenterologists. Patients should be allowed to have the choice between immediate colonoscopy and imaging surveillance for one or two isolated small polyps detected at colorectal cancer screening,' said Dr. Pickhardt.
CT colonography is now a recommended test for colorectal cancer screening by the American Cancer Society. 'If patients with small polyps are monitored, only five percent of adults undergoing CTC screening will need to undergo immediate invasive colonoscopy,' said Dr. Pickhardt.
This study appears in the November issue of the American Journal of Roentgenology.
Click here for abstract"
A decision analysis model was constructed to represent the clinical and economic consequences of performing three year colorectal cancer surveillance, immediate colonoscopy with polypectomy, or neither on patients who have 6-9 mm polyps found on CT colonography (CTC). The analysis model was accompanied by a hypothetical population of 100,000 60-year-old adults with 6- to 9-mm polyps detected at CTC screening. Results showed that, 'by excluding large polyps and masses, CTC screening can place a patient in a very low risk category making colonoscopy for small polyps probably not warranted,' said Perry J. Pickhardt, MD, lead author of the study. 'Approximately 10,000 colonoscopy referrals would be needed for each theoretical cancer death prevented at a cost of nearly $400,000 per life-year gained. We would also expect an additional 10 perforations and probably one death related to these extra colonoscopies. There may be no net gain in terms of lives - just extra costs,' said Dr. Pickhardt.
'The clinical management of small polyps detected at colorectal cancer screening has provoked controversy between radiologists and gastroenterologists. Patients should be allowed to have the choice between immediate colonoscopy and imaging surveillance for one or two isolated small polyps detected at colorectal cancer screening,' said Dr. Pickhardt.
CT colonography is now a recommended test for colorectal cancer screening by the American Cancer Society. 'If patients with small polyps are monitored, only five percent of adults undergoing CTC screening will need to undergo immediate invasive colonoscopy,' said Dr. Pickhardt.
This study appears in the November issue of the American Journal of Roentgenology.
Click here for abstract"
Virtual Colonoscopy: A Storm is Brewing
Virtual Colonoscopy: A Storm is Brewing
David J. Vining, MD Appl Radiol. 2008;37(11):12-16. ©2008 Anderson Publishing, Ltd.
Posted 11/11/2008
Abstract and Introduction
Abstract
The author performed the first virtual colonoscopy (VC) in 1993. In this article, he addresses the issues related to the turf battles between radiologists and gastroenterologists in the use of this technology. Reviewing common myths associated with VC, he warns that radiologists must retain expertise in this area.
Introduction
A storm is brewing around virtual colonoscopy (VC) and whether radiologists or gastroenterologists will ultimately control this technology. Imagine the following: in the near future, a patient who requires colorectal cancer (CRC) screening walks into a local gastroenterologist's office, obtains a VC examination, which is read by a nurse practitioner, and, following consultation with a gastroenterologist, undergoes immediate optical colonoscopy (OC) for evaluation of tiny polyps that either cannot be found or turn out to be residual feces. Meanwhile, a radiologist working with this practice interprets the CT data for extracolonic findings in exchange for a small percentage of the total professional fee. The patient's insurance (ie, Medicare) is billed for both the VC and OC, which taxpayers ultimately pay. If this sounds far-fetched, read on....
Virtual Colonoscopy Development
Colorectal cancer is the second leading cause of cancer death in the United States, but it is also one of the most preventable when screening is used to detect and treat early disease. The 5-year survival rate for early stage I CRC is 93%, but when it metastasizes to distant organs and becomes stage IV disease, the survival rate decreases to 8%.[1] Unfortunately, many adults over the age of 50 do not undergo screening, and, as a result, CRC is more often diagnosed in advanced stages.[2] Virtual colonoscopy offers the public a more appealing and less invasive alternative for screening.
I performed the first VC, also known as CT colonography (CTC), at the Wake Forest University Health Sciences Center in 1993. It has taken nearly 15 years for VC to mature and gain acceptance by policy makers. The basic technique consists of: 1) bowel cleansing and stool tagging, 2) gas insufflation of the colon, 3) CT scanning of the abdomen/pelvis, and 4) 2- and 3-dimensional image analysis of the data to identify polyps and masses (Figure 1). The first VC examination took 60 seconds to scan a patient using a single-slice helical CT scanner and nearly 8 hours to process the data for a fly-through, but today multidetector CT scanners acquire the data in a few seconds, and processing occurs in real time using inexpensive computers.
Figure 1.(A) This CT image shows a 10-mm polyp (arrow) on a fold in the sigmoid colon. (B) This 3-dimensional volume-rendered image shows the polyp (arrow) from a superior perspective.
Despite the technological advances that have occurred during the past decade (eg, CO2 insufflation, multidetector CT scanners, stool tagging, computer-assisted diagnosis), a strong lobbying effort on the part of gastroenterologists has delayed the availability of VC in the United States. Since Congress approved reimbursement for CRC screening in the 1997 Balanced Budget Act, the number of colonoscopies conducted annually in the United States has increased from 4 million in 2000 to >14 million in 2002.[3]
Handwriting on the Wall
Clinical trials that compared VC with OC have shown a dramatic improvement in VC accuracy in the last few years, culminating in 2 major trials that were announced in September 2007. The ACRIN National Colonography Trial enrolled over 2500 patients at 15 sites, and it reported that VC had a 90% sensitivity for the detection of polyps >10 mm.[4] Within a week, Kim[5] published a study comparing VC screening in 3120 patients with OC screening in 3163 patients. Remarkably, VC and OC found an equivalent number of advanced adenomas in each group; more surprisingly, a larger number of cancers were found in the VC group.[5] These 2 studies plus multiple prior published trials from the United States and abroad led the American Cancer Society, the American College of Radiology (ACR), and the United States Multi-Society Task Force to incorporate VC in its screening recommendations that were published in March 2008.[6]
As VC has gained acceptance, gastroenterologists now realize that VC will impact their practice. After years of bashing VC as not being good enough and requiring more clinical data, the Future Trends Committee of the American Gastroenterological Association (AGA) published a report in October 2006 stating that they see the handwriting on the wall.[7] This Committee proposed that gastroenterologists should position themselves to play a role in performing and interpreting VC, including advocating for CPT codes in the 91000 series that will allow gastroenterologists to be reimbursed for interpreting and providing VC services, as well as developing specialized training and training requirements for those interested in performing VC interpretation. In an effort to make good on its promise, the AGA published a set of guidelines in 2007 listing the minimum requirements that a gastroenterologist must satisfy in order to become certified to read VC examinations.[8]
Battle Lines are Drawn
Currently the Centers for Medicare and Medicaid Services (CMS) approve reimbursement for VC only when it follows a failed "diagnostic" colonoscopy, not a failed "screening" colonoscopy (Figure 2).[9] Following the inclusion of VC in the American Cancer Society's screening guidelines, CMS launched a National Coverage Analysis for Screening Computed Tomography Colonography for Colorectal Cancer (CAG-00396N) in May 2008. This seeks to expand reimbursement for screening indications. The final report of this analysis is due in February 2009.[10] Expanded reimbursement could have a huge impact on increasing screening and reducing CRC deaths, but it could also have substantial economic consequences for CMS and taxpayers. A public comment period held May-June 2008 drew responses from many individuals and organizations, including the ACR and the AGA. Of course, the ACR is in favor of expanded reimbursement, but the AGA stated that it would support VC only if certain conditions were met,[11] including:
Figure 2.(A) Virtual colonoscopy (VC) shows a diverticular stricture (right arrow) that prevented colonoscopy from successfully evaluating the entire colon. However, VC was able to identify an ascending colon cancer (left arrow) that was the cause of the patient's occult gastrointestinal bleeding. (B) A close-up of the ascending colon cancer from a superior view.
1. Reporting of ALL polyps (which is contradictory to the ACR Practice Guideline for the Performance of CTC in Adults that states reporting of polyps <5 mm is not recommended because of the low incidence of those lesions having malignant potential);[12]
2. Allowing patients in consultation with their physician to determine whether or not to remove those polyps; and
3. Enacting a coverage policy that would encourage rapid follow-up procedures (ie, colonoscopy) and that correspondingly would not create a disincentive for physicians (ie, gastroenterologists) who refer those procedures.
Reading between the lines, if such conditions are approved by CMS, then the gastroenterologists will have an unrestrained ability to perform colonoscopy on any little lump or bump that they might discover if they or their clinical assistant should be allowed to read VC exams. It is also the position of many prominent gastroenterologists to create a split-fee arrangement with radiologists so that radiologists will be relegated to reading only the extracolonic portions of a CT scan for a small portion of the professional fee, and, if radiologists refuse to participate, then they will outsource radiology services, even to foreign providers![13]
Dispelling Popular Myths
Gastroenterologists frequently try to discredit VC with the following myths:
1. Colonoscopy is the "gold standard." There are no published studies to validate this claim. In fact, studies comparing back-to-back colonoscopies on the same patients have reported OC miss rates of 22% for polyps, even in the hands of expert endoscopists.[14] Studies such as Pickhardt's[15] landmark VC study have shown VC to outperform OC. Finally, the accuracy of screening colonoscopy has been shown to be dependent on how much time a gastroenterologist spends performing the examination.[16]
2. If VC finds a polyp, then colonoscopy is needed for polyp removal, so why not undergo colonoscopy in the first place? The vast majority of polyps are benign, hyperplastic polyps, and <5% of the asymptomatic screening population has a significant adenomatous polyp.[5] Hence, if OC is the primary screening method, then >95% of the asymptomatic population would under go OC unnecessarily with its inherent risks of bowel perforation and anesthesia.
3. The radiation dose associated with VC is prohibitive. Radiation dose is a valid concern, but researchers are striving to mitigate this risk by using low-dose techniques, even as low as 10 mAs (compared with a conventional CT scan that might use a dose of 200 mAs).[17] Hence, the radiation risk from VC with low-dose techniques can be on the order of 1 to 2 mSv, which is far below the range that has been associated with potential cancer and multidetector CT use.[18] Alternatively, VC can be performed using MRI, but the availability of MRI scanners is a temporary hurdle, at least for today.
Actions to Take
Radiologists are already overworked due to the exponential increase in imaging studies during the past decade, and as a result, we have become complacent about the ownership of new technologies. In the meantime, gastroenterologists are purchasing CT scanners and attending training programs to get ready for CMS approval of reimbursement for VC screening.[19] However, if radiologists act quickly and take certain steps to position ourselves to maintain control of VC, we will not risk losing this technology, as we have done with cardiac imaging. Some initiatives include:
1. Taking a stronger, vocal interest in VC. Radiologists are better trained to read an entire CT examination, especially when disease crosses organ boundaries to involve both the colon and adjacent anatomy. We need to establish ourselves as the imaging experts in order to counter claims that endoscopists and nurse practitioners are as good as radiologists in reading VC exams.[20]
2. Beginning a dialogue with community gastroenterologists and primary care physicians. Radiology practices need to be willing to provide same-day, on-demand VC services for failed "diagnostic" colonoscopy examinations in advance of the anticipated reimbursement for screening VC.
3. Developing practice guidelines for appropriately working-up extracolonic findings. Perhaps offering immediate but limited ultrasound evaluation to resolve indeterminate liver and renal lesions will help to mitigate the gastroenterologists' cry that they should be the ones performing VC in their offices.
4. Providing consistent, high-quality reports of VC findings that can be rapidly delivered to the patient and referring clinician. Utilization of the CT Colonography Reporting and Data System (C-RADS) and participation in the ACR's CTC Registry will help to strengthen our position in the field.[21,22]
5. Challenging any proposals by gastroenterologists to split the professional fee for reading colonic and extracolonic portions of a VC CT scan, including legislative lobbying if necessary. There are many problems with fee-splitting arrangements, not the least of which is malpractice liability—radiologists will certainly be held liable when gastroenterologists fail to make a correct diagnosis if they should be allowed to interpret only the intraluminal portion of a VC scan.
All is Not Lost, at Least Not Yet
Much of the rhetoric coming from the gastroenterology community is coming from a few but very vocal and rabid gastroenterologists. In fact, a survey of 2400 AGA members regarding their interest in VC resulted in only 588 responses, of which one third said that they would want to perform VC, another third said that they would not perform it but would support their colleagues, and the final third said that gastroenterologists should not perform VC.[23] In reality, radiologists and gastroenterologists will need to work together along with surgeons and oncologists to provide comprehensive CRC screening and treatment services. If CRC screening really takes off, then there will not be enough gastroenterologists available in this country to perform the necessary therapeutic colonoscopies that will be generated. Although radiologists specializing in VC may eventually become employees of large, multispecialty clinics specializing in colorectal disease, it is paramount that the role and expertise of the radiologist be maintained.
--
www.hwsfinance.blogspot.com/
NAI
Unfortunately, nonaccidental trauma is common. More than 1 million children are seriously injured and 5000 killed secondary to abuse each year in the U.S. alone. Most children are younger than 1 year, and almost all are younger than 6 years.
In a child younger than two years of age, any suspicion of child abuse requires a skeletal survey and a head CT. In a child older than 2, symptom-specific imaging is recommended; brain MR or head CT can also be considered to evaluate for remote injury. Bone scan is sometimes useful, usually in the setting of equivocal radiographic findings or delayed workup. Bone scan is more sensitive for rib fractures, but less sensitive for skull and metaphyseal fractures.
Certain clinical findings should raise the suspicion of child abuse. These include multiple fractures, especially of different ages, bruising greater than expected for the patient's age, burns (often in the shape of common objects), bite marks, retinal hemorrhage, injury inconsistent with history, and delay in seeking care.
Fractures have varying levels of specificity for child abuse. The most common fracture in abuse is a long bone shaft fracture, which is not specific for abuse, except in infants younger than 9 months. Metaphyseal "bucket handle" or "corner" fractures have a high specificity for abuse. These occur most frequently at the knee (distal femur or proximal tibia and fibula), ankle (distal tibia) and shoulder (proximal humerus). Posterior rib fractures also have a high specificity. Rib fractures occur in 5-27% of abuse victims; 90% of all rib fractures occur in patients younger than 2 years. Other high specificity fractures include scapular and sternal fractures. Skull fractures are not well-correlated with abuse, as they are common in accidental trauma. Skull fracture findings concerning for abuse include multiple fractures and stellate fractures.
Brain injury is the leading cause of morbidity and mortality in nonaccidental trauma. Injury patterns include subarachnoid, subdural, and intraparenchymal hemorrhage. Diffuse cerebral edema and diffuse axonal injury can also be seen. An interhemispheric subdural hematoma is very concerning for abuse.
Abdominal injury related to child abuse primarily occurs in children older than 2. It is usually the result of blunt force trauma. It accounts for approximately 20% of the fatalities related to abuse. The most common finding is injury to the duodenum and proximal jejunum; mural hematoma may be seen. Another injury worthy of mention is pancreatitis; traumatic pancreatitis is the second most common etiology in kids. Other abdominal findings include solid organ lacerations and contusions, adrenal hematoma, and bladder rupture.
--
www.hwsfinance.blogspot.com/
In a child younger than two years of age, any suspicion of child abuse requires a skeletal survey and a head CT. In a child older than 2, symptom-specific imaging is recommended; brain MR or head CT can also be considered to evaluate for remote injury. Bone scan is sometimes useful, usually in the setting of equivocal radiographic findings or delayed workup. Bone scan is more sensitive for rib fractures, but less sensitive for skull and metaphyseal fractures.
Certain clinical findings should raise the suspicion of child abuse. These include multiple fractures, especially of different ages, bruising greater than expected for the patient's age, burns (often in the shape of common objects), bite marks, retinal hemorrhage, injury inconsistent with history, and delay in seeking care.
Fractures have varying levels of specificity for child abuse. The most common fracture in abuse is a long bone shaft fracture, which is not specific for abuse, except in infants younger than 9 months. Metaphyseal "bucket handle" or "corner" fractures have a high specificity for abuse. These occur most frequently at the knee (distal femur or proximal tibia and fibula), ankle (distal tibia) and shoulder (proximal humerus). Posterior rib fractures also have a high specificity. Rib fractures occur in 5-27% of abuse victims; 90% of all rib fractures occur in patients younger than 2 years. Other high specificity fractures include scapular and sternal fractures. Skull fractures are not well-correlated with abuse, as they are common in accidental trauma. Skull fracture findings concerning for abuse include multiple fractures and stellate fractures.
Brain injury is the leading cause of morbidity and mortality in nonaccidental trauma. Injury patterns include subarachnoid, subdural, and intraparenchymal hemorrhage. Diffuse cerebral edema and diffuse axonal injury can also be seen. An interhemispheric subdural hematoma is very concerning for abuse.
Abdominal injury related to child abuse primarily occurs in children older than 2. It is usually the result of blunt force trauma. It accounts for approximately 20% of the fatalities related to abuse. The most common finding is injury to the duodenum and proximal jejunum; mural hematoma may be seen. Another injury worthy of mention is pancreatitis; traumatic pancreatitis is the second most common etiology in kids. Other abdominal findings include solid organ lacerations and contusions, adrenal hematoma, and bladder rupture.
--
www.hwsfinance.blogspot.com/
Cerebral venous thrombosis
Discussion:
 Figure 2. (Click to enlarge) | 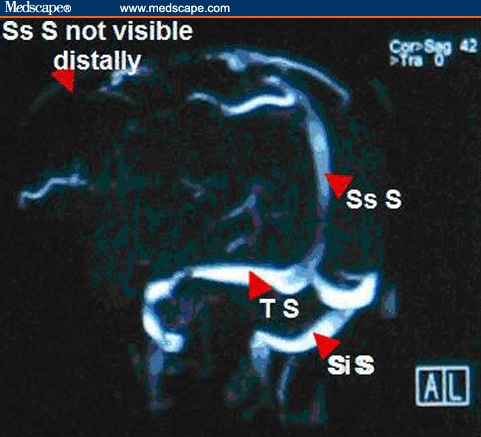 Figure 3. (Click to enlarge) |
Please note: in Figures 2 and 3, Ss S= Superior sagittal sinus, Co S= Confluence of sinus, Si S= Sigmoid sinus, and T S= Transverse sinus.
This patient had an MRV that showed a superior sagittal sinus thrombosis. Lack of signal from the distal portion of the superior sagittal sinus was consistent with cerebral venous thrombosis, as was the clinical presentation of this patient. A workup for a hypercoagulable state was negative. Cerebral venous thrombosis (CVT) should be considered in any patient presenting with severe headache and vomiting when no other cause is identified, especially when papilledema is identified on ophthalmoscopy. Risk factors for CVT include trauma (head injury), iatrogenic causes (craniotomy, jugular catheterization, lumbar puncture), systemic conditions (pregnancy, puerperium, dehydration), infections (otitis, sinusitis), inherited or acquired hypercoagulable states (protein C or S deficiency, antiphospholipid antibody syndrome, antithrombin III deficiency, factor V Leiden), collagen vascular diseases (systemic lupus erythematosus, Wegener granulomatosis), hematologic conditions (polycythemia, paroxysmal nocturnal hemoglobinuria, sickle cell disease), and medications (oral contraceptives, hormone therapy, steroids); however, no risk factors are identified in 14% of patients diagnosed with CVT.[6,7,8]
The typical pathophysiology in CVT is partial or complete occlusion of a cerebral venous sinus, which causes increased intracranial pressure and papilledema. The most frequently involved venous sinuses are the superior sagittal sinus or either of the paired transverse sinuses. If a thrombus extends into the cortical veins, dilatation of veins and capillary beds can occur, which then can lead to venous infarction, cerebral edema, and intraparenchymal hematoma formation. Seizures or cerebral herniation are potentially fatal complications.[7]
The clinical presentation of CVT is usually that of a severe headache that is aggravated by head movements, sneezing or coughing. The headache is typically subacute and gradual in onset, although thunderclap headache occurs in 2-10% of cases (as in this patient). Nausea and vomiting are often present, and severe cases are marked by a decreasing level of consciousness that may result from either a postictal state from seizures or from cerebral swelling with or without herniation. Focal neurologic findings, including hemiparesis or isolated unilateral lower extremity weakness, can be seen when a thrombus extends into the cortical veins. This is especially common in CVT of the superior sagittal sinus. If the cavernous sinus is involved (which is almost exclusively associated with infection of the paranasal sinuses), proptosis and chemosis with ipsilateral periorbital edema, retinal hemorrhages, papilledema, extraocular movement abnormalities, and sensory loss in the V1 or V2 distribution of the trigeminal nerve may be seen. Isolated or multiple cranial nerve palsies (III, VII, VIII) have been reported in patients with unilateral occlusion of the transverse or sigmoid sinuses. This unusual presentation has been explained by venous congestion of the ventral pontine and lateral medullary veins. If the thrombus extends into the jugular bulb, a jugular foramen syndrome, with involvement of cranial nerves IX, X and XI, may be seen. The physical examination is normal in 15-30% of patients, although careful examination may reveal loss of normal spontaneous retinal venous pulsations. It has been has reported that headache (89%), paresis (37%), generalized (30%) or focal (20%) seizures, papilledema (28%), and mental status changes (22%) are the most frequent presenting symptoms and signs associated with the diagnosis of CVT.[1,6,7,8]
The differential diagnosis of CVT includes subarachnoid hemorrhage, intracranial hemorrhage, ischemic stroke, and bacterial meningitis. In patients presenting with the more typical subacute onset, pseudotumor cerebri, cavernous sinus syndromes, intracranial abscess, subdural empyema, and brain tumor should be considered.[7,8]
The definitive diagnosis of CVT is demonstration of the thrombus by neuroimaging. Noncontrast-enhanced CT scans of the head are normal in 25% of patients with a normal examination and 10% of patients with focal neurologic findings (including papilledema). The delta sign is a dense triangle in the superior sagittal sinus caused by the thrombus, and it may be seen on CT scans. MRV is considered the radiographic investigation of choice and will demonstrate areas of lack of signal where the thrombus involves the venous sinuses. Cerebral angiography may be required if MRV is non-diagnostic and suspicion remains high. CT venography is a method that is increasingly being used to diagnose CVT, and it has been shown to be very sensitive and specific. The empty delta sign is a triangular filling defect in the superior sagittal sinus that complements the delta sign on noncontrast-enhanced CT scans. Lumbar punctures are sometimes performed in patients with no evidence of mass effect on CT scans. About 50% of patients will have abnormal cerebrospinal fluid (CSF) findings, including mild lymphocytic pleocytosis, elevated protein, the presence of red blood cells, and, more commonly, an elevated CSF opening pressure (which must be measured with the patient as relaxed as possible in the lateral decubitus position).[3,4,6,7,8]
The mainstay of treatment for CVT, even in patients with CT evidence of cerebral ischemia or hemorrhage, is anticoagulation. In 2 retrospective studies of patients with CVT and moderate-sized hematomas, anticoagulation was not associated with increased hemorrhage volume, neurologic deterioration, or a worse outcome. Heparin should be started initially, with a goal of maintaining an activated partial thromboplastin time that is twice the control value. Heparin therapy is gradually transitioned to warfarin, which is then continued for 4-6 months (longer in patients with an identified predisposition to clotting). Endovascular thrombolytic therapy with urokinase or tissue plasminogen activator (tPA) may be effective in patients who deteriorate despite adequate anticoagulation with heparin, but this therapy is limited to specialized centers. Surgical intervention, in the form of a thrombectomy using a microsnare or rheolytic thrombectomy catheter with local thrombolytic therapy, has been used with variable success in the setting of severe neurologic deterioration. Adjunctive therapy for seizures, cerebral edema or co-occurring infections may also be required on a case-by-case basis. Headaches related to increased intracranial pressure may respond to elevation of the head of the bed or to acetazolamide, which decreases CSF production (thereby lowering intracranial pressure). When complicated by visual deterioration unresponsive to these measures, lumboperitoneal shunting or optic nerve sheath fenestration should be considered.[4,6,7]
The complications of CVT may include coma (resulting from status epilepticus, critically elevated intracranial pressure, or impending cerebral herniation) and pulmonary embolism. In patients who are comatose as a result of raised intracranial pressure, prompt intervention is critical. Initial measures include maintaining the head of the patient at 30-40° elevation, keeping the neck in a neutral position to avoid kinking of the jugular veins, and the use of mannitol or hyperventilation. Additional therapy, such as ventriculostomy and blood pressure titration with vasoactive agents, should be guided by direct intracranial pressure monitoring. Pulmonary embolisms occur in up to 11% of cases and may originate from the thrombosed jugular veins or from other sites (such as the legs). This complication carries a high mortality rate.
The prognosis is good for patients with CVT that is recognized early. Full recovery is expected in about 70% of cases. Of the remaining 30%, about one third die and two thirds are left with persistent mild-to-moderate neurologic deficits. Coma, seizures, or underlying disease have no significant effect on the short-term outcome and should not preclude any type of therapeutic intervention. The long-term recurrence rate of CVT is approximately 20%. Oral contraceptives are a recognized risk factor for CVT; this is supported by the increasing rate of CVT in women of childbearing age since introduction of oral contraceptives, with stable rates seen in men of similar age.[7]
In the case presented above, the patient was treated with analgesics and low-molecular-weight heparin, followed by warfarin. She discontinued use of her oral contraceptive pills. The patient recovered completely, with no residual deficits, and she continues to do well on long-term follow-up.
--
www.hwsfinance.blogspot.com/
Monday, November 10, 2008
MRI of Temporomandibular Joint Disorders
Sent to you by Hemi via Google Reader:
via Medscape Radiology Headlines on 7/10/08
Magnetic resonance imaging (MRI) plays an important role in the evaluation of temporomandibular disorders (TMD). What are the MRI appearances of the degenerated temporomandibular joint? Applied Radiology
Things you can do from here:
- Subscribe to Medscape Radiology Headlines using Google Reader
- Get started using Google Reader to easily keep up with all your favorite sites
Proximal Vein Compressibility on Ultrasound Sufficient for Diagnosing DVT
Sent to you by Hemi via Google Reader:
via Medscape Radiology Headlines on 8/10/08
For symptomatic outpatients with suspected deep vein thrombosis (DVT) of the lower extremities, results of a prospective clinical trial suggest that "2-point ultrasonography," or "compression ultrasonography," evaluating compressibility of the proximal veins is as accurate as whole-leg Doppler ultrasonography. Reuters Health Information
Things you can do from here:
- Subscribe to Medscape Radiology Headlines using Google Reader
- Get started using Google Reader to easily keep up with all your favorite sites
Radiological Case: Pigmented Villonodular Synovitis of the Elbow
Sent to you by Hemi via Google Reader:
via Medscape Radiology Headlines on 13/10/08
Increasing elbow pain and swelling were present in a 73-year-old woman who was diagnosed with pigmented villonodular synovitis of the elbow. What was the preferred diagnostic imaging modality? Things you can do from here:
- Subscribe to Medscape Radiology Headlines using Google Reader
- Get started using Google Reader to easily keep up with all your favorite sites
Radiological Case: Budd-Chiari Syndrome
Sent to you by Hemi via Google Reader:
via Medscape Radiology Headlines on 21/10/08
Right upper quadrant pain was present in a 77-year-old woman who was diagnosed with Budd-Chiari syndrome. Which imaging modalities were used to evaluate her pain and diagnose her condition? Applied Radiology
Things you can do from here:
- Subscribe to Medscape Radiology Headlines using Google Reader
- Get started using Google Reader to easily keep up with all your favorite sites
CT Important in Emergency Diagnosis of Appendicitis
Sent to you by Hemi via Google Reader:
via Medscape Radiology Headlines on 31/10/08
CT of the appendix has a significant impact on the management of emergency department patients who are suspected of having appendicitis, researchers report in the October issue of the American Journal of Roentgenology. Reuters Health Information
Things you can do from here:
- Subscribe to Medscape Radiology Headlines using Google Reader
- Get started using Google Reader to easily keep up with all your favorite sites
Online Radiological Case: Idiopathic Epidural Lipomatosis
Sent to you by Hemi via Google Reader:
via Medscape Radiology Headlines on 31/10/08
A history of compressive myelopathy is present in a 35-year-old man diagnosed with idiopathic epidural lipomatosis. What's the preferred imaging modality for diagnosis and follow-up of this condition? Applied Radiology
Things you can do from here:
- Subscribe to Medscape Radiology Headlines using Google Reader
- Get started using Google Reader to easily keep up with all your favorite sites
Facet Joint Osteoarthritis and Low Back Pain in the Community-Based Population
Sent to you by Hemi via Google Reader:
via Medscape Radiology Headlines on 7/11/08
Is there an association between lumbar spine facet joint osteoarthritis and low back pain? See the results from this community-based Framingham Heart Study. Spine
Things you can do from here:
- Subscribe to Medscape Radiology Headlines using Google Reader
- Get started using Google Reader to easily keep up with all your favorite sites
Thursday, November 6, 2008
 (TNF-
(TNF-
































Subscribe to:
Posts (Atom)

