Discussion:
 Figure 2. (Click to enlarge) | 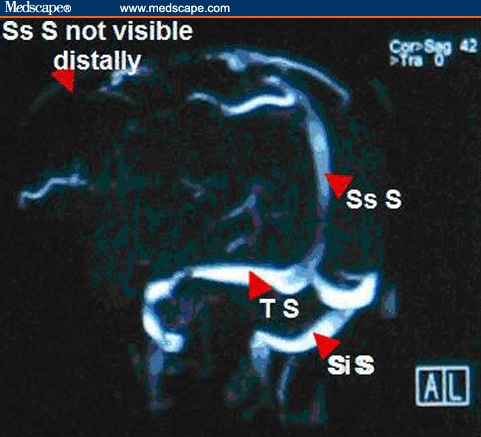 Figure 3. (Click to enlarge) |
Please note: in Figures 2 and 3, Ss S= Superior sagittal sinus, Co S= Confluence of sinus, Si S= Sigmoid sinus, and T S= Transverse sinus.
This patient had an MRV that showed a superior sagittal sinus thrombosis. Lack of signal from the distal portion of the superior sagittal sinus was consistent with cerebral venous thrombosis, as was the clinical presentation of this patient. A workup for a hypercoagulable state was negative. Cerebral venous thrombosis (CVT) should be considered in any patient presenting with severe headache and vomiting when no other cause is identified, especially when papilledema is identified on ophthalmoscopy. Risk factors for CVT include trauma (head injury), iatrogenic causes (craniotomy, jugular catheterization, lumbar puncture), systemic conditions (pregnancy, puerperium, dehydration), infections (otitis, sinusitis), inherited or acquired hypercoagulable states (protein C or S deficiency, antiphospholipid antibody syndrome, antithrombin III deficiency, factor V Leiden), collagen vascular diseases (systemic lupus erythematosus, Wegener granulomatosis), hematologic conditions (polycythemia, paroxysmal nocturnal hemoglobinuria, sickle cell disease), and medications (oral contraceptives, hormone therapy, steroids); however, no risk factors are identified in 14% of patients diagnosed with CVT.[6,7,8]
The typical pathophysiology in CVT is partial or complete occlusion of a cerebral venous sinus, which causes increased intracranial pressure and papilledema. The most frequently involved venous sinuses are the superior sagittal sinus or either of the paired transverse sinuses. If a thrombus extends into the cortical veins, dilatation of veins and capillary beds can occur, which then can lead to venous infarction, cerebral edema, and intraparenchymal hematoma formation. Seizures or cerebral herniation are potentially fatal complications.[7]
The clinical presentation of CVT is usually that of a severe headache that is aggravated by head movements, sneezing or coughing. The headache is typically subacute and gradual in onset, although thunderclap headache occurs in 2-10% of cases (as in this patient). Nausea and vomiting are often present, and severe cases are marked by a decreasing level of consciousness that may result from either a postictal state from seizures or from cerebral swelling with or without herniation. Focal neurologic findings, including hemiparesis or isolated unilateral lower extremity weakness, can be seen when a thrombus extends into the cortical veins. This is especially common in CVT of the superior sagittal sinus. If the cavernous sinus is involved (which is almost exclusively associated with infection of the paranasal sinuses), proptosis and chemosis with ipsilateral periorbital edema, retinal hemorrhages, papilledema, extraocular movement abnormalities, and sensory loss in the V1 or V2 distribution of the trigeminal nerve may be seen. Isolated or multiple cranial nerve palsies (III, VII, VIII) have been reported in patients with unilateral occlusion of the transverse or sigmoid sinuses. This unusual presentation has been explained by venous congestion of the ventral pontine and lateral medullary veins. If the thrombus extends into the jugular bulb, a jugular foramen syndrome, with involvement of cranial nerves IX, X and XI, may be seen. The physical examination is normal in 15-30% of patients, although careful examination may reveal loss of normal spontaneous retinal venous pulsations. It has been has reported that headache (89%), paresis (37%), generalized (30%) or focal (20%) seizures, papilledema (28%), and mental status changes (22%) are the most frequent presenting symptoms and signs associated with the diagnosis of CVT.[1,6,7,8]
The differential diagnosis of CVT includes subarachnoid hemorrhage, intracranial hemorrhage, ischemic stroke, and bacterial meningitis. In patients presenting with the more typical subacute onset, pseudotumor cerebri, cavernous sinus syndromes, intracranial abscess, subdural empyema, and brain tumor should be considered.[7,8]
The definitive diagnosis of CVT is demonstration of the thrombus by neuroimaging. Noncontrast-enhanced CT scans of the head are normal in 25% of patients with a normal examination and 10% of patients with focal neurologic findings (including papilledema). The delta sign is a dense triangle in the superior sagittal sinus caused by the thrombus, and it may be seen on CT scans. MRV is considered the radiographic investigation of choice and will demonstrate areas of lack of signal where the thrombus involves the venous sinuses. Cerebral angiography may be required if MRV is non-diagnostic and suspicion remains high. CT venography is a method that is increasingly being used to diagnose CVT, and it has been shown to be very sensitive and specific. The empty delta sign is a triangular filling defect in the superior sagittal sinus that complements the delta sign on noncontrast-enhanced CT scans. Lumbar punctures are sometimes performed in patients with no evidence of mass effect on CT scans. About 50% of patients will have abnormal cerebrospinal fluid (CSF) findings, including mild lymphocytic pleocytosis, elevated protein, the presence of red blood cells, and, more commonly, an elevated CSF opening pressure (which must be measured with the patient as relaxed as possible in the lateral decubitus position).[3,4,6,7,8]
The mainstay of treatment for CVT, even in patients with CT evidence of cerebral ischemia or hemorrhage, is anticoagulation. In 2 retrospective studies of patients with CVT and moderate-sized hematomas, anticoagulation was not associated with increased hemorrhage volume, neurologic deterioration, or a worse outcome. Heparin should be started initially, with a goal of maintaining an activated partial thromboplastin time that is twice the control value. Heparin therapy is gradually transitioned to warfarin, which is then continued for 4-6 months (longer in patients with an identified predisposition to clotting). Endovascular thrombolytic therapy with urokinase or tissue plasminogen activator (tPA) may be effective in patients who deteriorate despite adequate anticoagulation with heparin, but this therapy is limited to specialized centers. Surgical intervention, in the form of a thrombectomy using a microsnare or rheolytic thrombectomy catheter with local thrombolytic therapy, has been used with variable success in the setting of severe neurologic deterioration. Adjunctive therapy for seizures, cerebral edema or co-occurring infections may also be required on a case-by-case basis. Headaches related to increased intracranial pressure may respond to elevation of the head of the bed or to acetazolamide, which decreases CSF production (thereby lowering intracranial pressure). When complicated by visual deterioration unresponsive to these measures, lumboperitoneal shunting or optic nerve sheath fenestration should be considered.[4,6,7]
The complications of CVT may include coma (resulting from status epilepticus, critically elevated intracranial pressure, or impending cerebral herniation) and pulmonary embolism. In patients who are comatose as a result of raised intracranial pressure, prompt intervention is critical. Initial measures include maintaining the head of the patient at 30-40° elevation, keeping the neck in a neutral position to avoid kinking of the jugular veins, and the use of mannitol or hyperventilation. Additional therapy, such as ventriculostomy and blood pressure titration with vasoactive agents, should be guided by direct intracranial pressure monitoring. Pulmonary embolisms occur in up to 11% of cases and may originate from the thrombosed jugular veins or from other sites (such as the legs). This complication carries a high mortality rate.
The prognosis is good for patients with CVT that is recognized early. Full recovery is expected in about 70% of cases. Of the remaining 30%, about one third die and two thirds are left with persistent mild-to-moderate neurologic deficits. Coma, seizures, or underlying disease have no significant effect on the short-term outcome and should not preclude any type of therapeutic intervention. The long-term recurrence rate of CVT is approximately 20%. Oral contraceptives are a recognized risk factor for CVT; this is supported by the increasing rate of CVT in women of childbearing age since introduction of oral contraceptives, with stable rates seen in men of similar age.[7]
In the case presented above, the patient was treated with analgesics and low-molecular-weight heparin, followed by warfarin. She discontinued use of her oral contraceptive pills. The patient recovered completely, with no residual deficits, and she continues to do well on long-term follow-up.
--
www.hwsfinance.blogspot.com/


No comments:
Post a Comment